Dehydration
In physiology, dehydration is a deficit of total body water, leading to the disruption of metabolic processes. It occurs when free water loss exceeds free water intake, usually due to exercise, disease, or high environmental temperature. Mild dehydration can also be caused by immersion diuresis, which may increase the risk of decompression sickness in divers.
Most people can tolerate a 3-4% decrease in total body water without difficulty or adverse health effects. A 5-8% decrease can cause fatigue and dizziness. Loss of over 10% of total body water can cause physical and mental deterioration, accompanied by severe thirst. Death occurs at a loss of between 15 and 25% of the body water. Mild dehydration is characterised by thirst and general discomfort and is usually resolved with oral rehydration.
Signs and Symptoms
The hallmarks of dehydration include thirst and neurological changes such as headaches, general discomfort, loss of appetite, nausea, decreased urine volume, confusion, unexplained tiredness, purple fingernails, and seizures. The symptoms become increasingly severe with greater total body water loss. Mild dehydration (1-2% body water loss) impairs cognitive performance. In people over age 50, the body's thirst sensation diminishes with age, but fluid intake does not differ significantly between young and old people. Dehydration is a significant concern in the elderly, especially during conditions that promote insensible free water losses, such as hot weather.

Causes
Dehydration can result from various factors, including physical exertion in hot and humid weather, high altitudes, endurance athletics, and chronic illnesses. It can also be a side effect of many medications. In the elderly, a blunted response to thirst or inadequate access to free water, particularly in the face of excess free water losses (especially hyperglycaemia), are primary causes. Water can leave the body through sensible losses such as osmotic diuresis, sweating, vomiting, and diarrhoea, and insensible losses through the skin and respiratory tract.
Diagnosis
Definition
Dehydration occurs when water intake does not replace free water lost due to normal physiological processes like breathing, urination, perspiration, or other causes like diarrhoea and vomiting. Severe dehydration can be life-threatening, leading to seizures or respiratory arrest, and carries the risk of osmotic cerebral oedema if rehydration is too rapid. It's essential to distinguish dehydration from hypovolaemia, which specifically refers to a decrease in blood plasma volume.
Physical Examination
The skin turgor test supports the diagnosis of dehydration. This test involves pinching the patient's skin and observing how quickly it returns to its normal position. However, the skin turgor test can be unreliable in patients with reduced skin elasticity, such as the elderly.
Prevention
For routine activities, thirst is generally an adequate guide to maintain proper hydration. Minimum water intake varies individually based on factors like weight, energy expenditure, age, sex, physical activity, environment, diet, and genetics. Additional water may be required with exercise, hot environments, or a decreased thirst response. In athletes, drinking to thirst optimises performance and safety. During heavy exertion or in warm weather, water loss can significantly increase due to sweating. Including sodium in fluid replacement drinks poses little or no risk and may have theoretical benefits, provided these fluids are hypotonic.
Treatment
The most effective treatment for minor dehydration is drinking water and reducing fluid loss. Plain water restores only the blood plasma volume, inhibiting the thirst mechanism before solute levels can be replenished. Solid foods can help replace fluid loss from vomiting and diarrhoea. Urine concentration and frequency will return to normal as dehydration resolves.
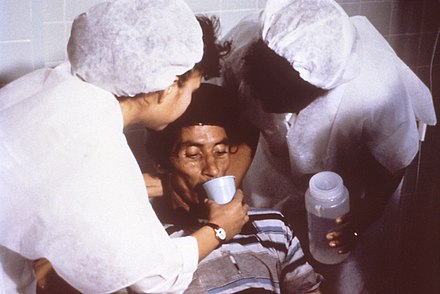
Oral rehydration therapy or intravenous fluid replacement may be necessary in some cases. Oral rehydration is less painful, non-invasive, inexpensive, and easier to provide, making it the treatment of choice for mild dehydration. Solutions used for intravenous rehydration must be isotonic or hypertonic, as pure water injected into veins can cause red blood cell lysis. In severe dehydration cases, fluids with a proper balance of replacement electrolytes are given orally or intravenously, with continuous assessment of electrolyte status. Complete resolution is typical in all but the most extreme cases.
Self-assessment MCQs (single best answer)
What is dehydration primarily characterised by?

At what percentage of total body water loss can physical and mental deterioration occur?
Which symptom is NOT typically associated with mild dehydration?
Which test is used to support the diagnosis of dehydration?
In the elderly, why is dehydration a significant concern?
What is the primary treatment for minor dehydration?
Which of the following is a potential cause of dehydration?
Why is oral rehydration therapy often preferred over intravenous fluids for mild dehydration?
Which of the following can be a side effect of many medications, leading to dehydration?
What can happen if rehydration is too rapid in cases of severe dehydration?
Dentaljuce
Dentaljuce provides Enhanced Continuing Professional Development (CPD) with GDC-approved Certificates for dental professionals worldwide.
Founded in 2009 by the award-winning Masters team from the School of Dentistry at the University of Birmingham, Dentaljuce has established itself as the leading platform for online CPD.
With over 100 high-quality online courses available for a single annual membership fee, Dentaljuce offers comprehensive e-learning designed for busy dental professionals.
The courses cover a complete range of topics, from clinical skills to patient communication, and are suitable for dentists, nurses, hygienists, therapists, students, and practice managers.
Dentaljuce features Dr. Aiden, a dentally trained AI-powered personal tutor available 24/7 to assist with queries and provide guidance through complex topics, enhancing the learning experience.
Check out our range of courses, or sign up now!