Golfer's elbow
Golfer's elbow, also known as medial epicondylitis, is a tendinosis affecting the medial common flexor tendon on the inside of the elbow. This condition is similar to tennis elbow, which affects the lateral epicondyle on the outside of the elbow. The pathology involves repetitive stress on the tendons, leading to microtears and tendon degeneration rather than acute inflammation.
Description
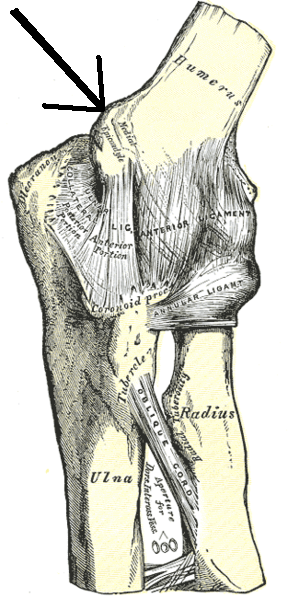
The anterior-medial forearm houses several muscles responsible for wrist flexion and forearm pronation. These include the pronator teres, flexor carpi radialis, palmaris longus, and flexor digitorum superficialis, all originating from the medial epicondyle of the humerus and innervated by the median nerve. The flexor carpi ulnaris, also attaching to the medial epicondyle, is innervated by the ulnar nerve. These muscles share a common tendinous attachment at the medial epicondyle, forming the flexor tendon, which is approximately 3 centimetres long and runs parallel to the ulnar collateral ligament.
Golfer's elbow is a chronic condition arising from repetitive arm movements, resulting in recurrent microtears within the flexor tendon. These microtears lead to collagen remodelling and an increase in mucoid ground substance, causing scar tissue formation and tendon thickening, ultimately reducing collagen strength and leading to pain with repetitive use.
Causes

The term "golfer's elbow" originates from the pain experienced during a full golf swing, specifically from the top of the backswing to just before ball impact. The motion generates high energy valgus forces during the late cocking (backswing in golf) and acceleration phase (downswing and impact). Similar stress on the tendon from repetitive throwing motions, such as in baseball or football, can also lead to the condition, sometimes referred to as "pitcher's elbow".
In adults, the pathophysiology may involve mucoid degeneration, characterised by disorganised collagen, increased extracellular matrix, and chondroid metaplasia. It remains unclear whether this condition is more common among individuals with forceful repetitive occupations compared to the general population.
Diagnosis
Medial epicondylitis is diagnosed through clinical evaluation, where characteristic pain is elicited during activities requiring wrist flexion strength. Physical examination reveals discrete point tenderness over the medial epicondyle and pain with resisted wrist flexion and passive wrist extension. Imaging such as radiography, ultrasound, and MRI may show calcifications or mucoid degeneration but are not essential for diagnosis.
Occurrence
Golfer's elbow affects approximately 0.4% of the population, predominantly occurring in individuals aged 45 to 64 and more frequently in women. Around 75% of cases involve the dominant arm. Risk factors include improper technique, lack of strength, endurance, or flexibility, and in manual labourers, heavy and repetitive activity, high body mass index, comorbidities, and high work demands.
Treatment
Initial treatment aims to alleviate pain through methods such as non-steroidal anti-inflammatory drugs (NSAIDs) like ibuprofen, naproxen, or aspirin, and the application of heat or ice. A counterforce brace or "elbow strap" may provide additional relief.
Conservative treatment often begins with rest, ice, compression, and elevation (R.I.C.E.), followed by therapy with an occupational therapist. Simple analgesics and oral anti-inflammatory medications help manage pain and inflammation. More invasive treatments include glucocorticoid injections into the affected area.
Physical Therapy
Therapeutic exercises focus on muscle and tendon reconditioning, starting with stretching and gradual strengthening of the flexor-pronator muscles. Initial strengthening involves isometrics, progressing to eccentric exercises to restore the range of motion. Post-exercise icing is common practice.
Surgery
Surgical intervention is considered after six months of unsuccessful conservative treatment. Common procedures include surgical debridement and ulnar nerve decompression. While most patients recover with rest, ice, and rehabilitative exercises, less than 10% require surgery. Arthroscopy is not an option for treating golfer's elbow.
Self-assessment MCQs (single best answer)
What is Golfer's Elbow also known as?

Which tendon is primarily affected in Golfer's Elbow?
Which muscle is NOT innervated by the median nerve in the context of Golfer's Elbow?
What is the primary cause of Golfer's Elbow?
What is a common non-surgical treatment for Golfer's Elbow?
Which imaging technique is NOT typically necessary for diagnosing Golfer's Elbow?
What percentage of Golfer's Elbow cases involve the dominant arm?
Which of the following is NOT a common risk factor for developing Golfer's Elbow?
What is the main goal of physical therapy in treating Golfer's Elbow?
What is the last resort treatment for Golfer's Elbow if conservative treatments fail?
Dentaljuce
Dentaljuce provides Enhanced Continuing Professional Development (CPD) with GDC-approved Certificates for dental professionals worldwide.
Founded in 2009 by the award-winning Masters team from the School of Dentistry at the University of Birmingham, Dentaljuce has established itself as the leading platform for online CPD.
With over 100 high-quality online courses available for a single annual membership fee, Dentaljuce offers comprehensive e-learning designed for busy dental professionals.
The courses cover a complete range of topics, from clinical skills to patient communication, and are suitable for dentists, nurses, hygienists, therapists, students, and practice managers.
Dentaljuce features Dr. Aiden, a dentally trained AI-powered personal tutor available 24/7 to assist with queries and provide guidance through complex topics, enhancing the learning experience.
Check out our range of courses, or sign up now!