Papillary Tumours of the Pineal Region
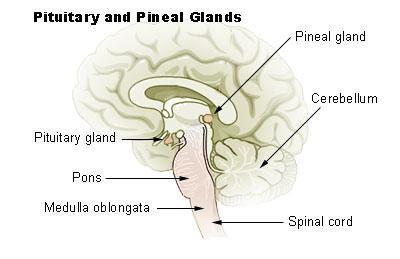
Papillary tumours of the pineal region were first described by A. Jouvet et al. in 2003 and were included in the World Health Organisation (WHO) classification of central nervous system tumours in 2007. These tumours are located on the pineal gland, a small, cone-shaped structure in the centre of the brain, situated on the roof of the diencephalon and dorsal to the midbrain tectum. The tumour appears to derive from the specialised ependymal cells of the subcommissural organ. Diagnosing these rare tumours is challenging due to their rarity.
Symptoms and Signs
The most common symptom of papillary tumours of the pineal region is a headache. Headaches occur secondary to hydrocephalus, resulting from compression of the cerebral aqueduct, a narrow channel in the midbrain connecting the third and fourth ventricles. When a tumour obstructs the cerebrospinal fluid pathway, it causes headaches. Persistent headaches often prompt patients to seek medical help. A shunt is sometimes placed to alleviate pressure caused by hydrocephalus, and in some cases, endoscopic third ventriculostomy is performed. Other symptoms may include progressive diplopia (double vision), nausea, and vomiting.
Pathology

Papillary tumours in the pineal region are composed of a variety of cells, including astrocytes, ganglion cells, blood vessels, and pinealocytes. Pinealocytes are specialised neurons rich in neurotransmitters like serotonin, norepinephrine, and melatonin. Papillary tumours are made up of ependymal cells forming papillae, which are surface cells lining the brain's ventricles. The tumour cells contain proteins from blood vessels, nerve cells, and muscle cells. These tumours have no known predisposing genetic characteristics, although they result from genetic mutations causing cells to divide abnormally.
Papillary tumours are typically well circumscribed and fairly large, ranging between 2.5 and 4.0 centimetres. They may feature a cystic component.
Histological and Immunohistochemical Features
Diagnosing papillary tumours can be difficult due to their similarity to other papillary lesions in the pineal region, such as parenchymal pineal tumours, papillary ependymoma, papillary meningioma, choroid plexus papilloma, and metastatic papillary carcinoma.
Papillary tumours typically show a discrete, compressive border with adjacent pineal gland and brain parenchyma. The tumour cells characteristically exhibit columnar to cuboidal cytoplasm with well-defined cytoplasmic membranes, and vacuolated, or clear cells are common. Necrosis is usually observed to some extent.
The immunohistochemical profile for papillary tumours includes the following markers:
- CK8/18 (cytokeratin 8/18): +++
- GFAP (glial fibrillary acidic protein): +
- NSE (neuron-specific enolase): ++
- CD56/N-CAM (neural cell adhesion molecule): ++
- S100: ++
- Vimentin: +
The intensity of immunoreactivity is scored as absent (-), weak/focal (+), moderate (++), and strong (+++).
Diagnosis
Grading

Papillary tumours of the pineal region are graded according to the WHO classification. Initially, they were classified as either malignant or benign. Now, they are graded as either Grade II or Grade III.
Grade II
Grade II tumours are relatively slow-growing, with slightly abnormal microscopic appearances and can spread into nearby normal tissue. They can recur as higher-grade tumours.
Grade III
Grade III tumours are malignant, with cells actively reproducing abnormal cells. These tumours often grow into nearby normal brain tissue and tend to recur as higher-grade tumours.
Epidemiology
Papillary tumours of the pineal region are extremely rare, constituting 0.4-1% of all central nervous system tumours. They most commonly occur in adults, with a mean age of 31.5 years, but have been reported in individuals aged 5 to 66 years. There is a slight predominance of females.
Current Research
Due to the rarity of these tumours, much remains unknown. Seventy cases have been published in English literature since 2003. Treatment guidelines have yet to be established, and a larger number of cases with longer clinical follow-ups are needed to optimise management. Gross total resection has been the only clinical factor associated with overall and progression-free survival. The value of radiotherapy and chemotherapy on disease progression requires further investigation.
Self-assessment MCQs (single best answer)
Who first described papillary tumours of the pineal region?

What is the most common symptom of papillary tumours of the pineal region?
What procedure might be performed to alleviate hydrocephalus caused by a papillary tumour?
Which type of cells are primarily involved in papillary tumours of the pineal region?
Which immunohistochemical marker shows strong (+++) intensity in papillary tumours of the pineal region?
How are papillary tumours of the pineal region graded according to the WHO classification?
What is the mean age at which papillary tumours of the pineal region most commonly occur?
What is the percentage of papillary tumours of the pineal region among all central nervous system tumours?
Which histological feature is commonly observed in papillary tumours of the pineal region?
What is the only clinical factor associated with overall and progression-free survival in papillary tumours of the pineal region?
Dentaljuce
Dentaljuce provides Enhanced Continuing Professional Development (CPD) with GDC-approved Certificates for dental professionals worldwide.
Founded in 2009 by the award-winning Masters team from the School of Dentistry at the University of Birmingham, Dentaljuce has established itself as the leading platform for online CPD.
With over 100 high-quality online courses available for a single annual membership fee, Dentaljuce offers comprehensive e-learning designed for busy dental professionals.
The courses cover a complete range of topics, from clinical skills to patient communication, and are suitable for dentists, nurses, hygienists, therapists, students, and practice managers.
Dentaljuce features Dr. Aiden, a dentally trained AI-powered personal tutor available 24/7 to assist with queries and provide guidance through complex topics, enhancing the learning experience.
Check out our range of courses, or sign up now!