Pulmonary Hypertension
Pulmonary hypertension (PH) is a medical condition characterised by increased blood pressure in the arteries of the lungs. This condition can present with symptoms such as shortness of breath, chest pain, fatigue, swelling of the legs, and a fast heartbeat. The condition impairs the ability to exercise and worsens gradually.
According to the 6th World Symposium on Pulmonary Hypertension in 2018, PH is diagnosed when the pulmonary mean arterial pressure exceeds 20mmHg at rest, and pulmonary vascular resistance is greater than 3 Wood units.
Classification
Pulmonary hypertension is classified into five groups by the WHO, with Group I being further subdivided. Group I includes pulmonary arterial hypertension (PAH), with idiopathic, heritable, and drug/toxin-induced forms. Group II is associated with left heart disease, Group III with lung disease and hypoxia, Group IV with chronic arterial obstructions, and Group V with multifactorial mechanisms.
Signs and Symptoms
The primary symptoms include shortness of breath, fatigue, chest pain, palpitations, right-sided abdominal pain, poor appetite, lightheadedness, fainting, and swelling of the legs or ankles. Cyanosis, non-productive cough, and exercise-induced nausea are less common symptoms. Typical physical signs include an accentuated pulmonary component of the second heart sound, right ventricular third heart sound, and parasternal heave, indicating a hypertrophied right ventricle.
Causes
The exact cause of pulmonary hypertension often remains unidentified. Risk factors include family history, pulmonary embolism, HIV/AIDS, sickle cell disease, cocaine use, chronic obstructive pulmonary disease (COPD), sleep apnoea, and living at high altitudes. The condition results from inflammation and subsequent remodelling of the lung arteries, making it challenging for the heart to pump blood through the lungs.
Pathogenesis
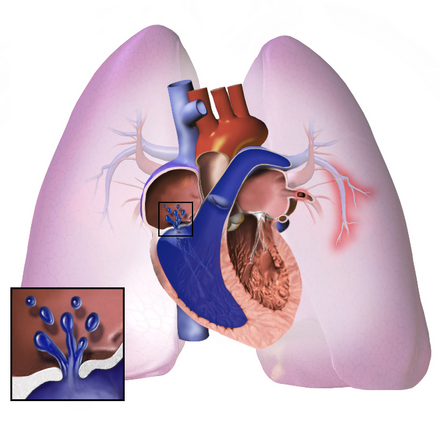
The pathogenesis of PAH involves the narrowing of blood vessels within the lungs, leading to increased pressure and workload on the right side of the heart. Over time, blood vessels thicken and stiffen, further elevating pulmonary blood pressure and reducing blood flow. This condition ultimately results in right heart failure.

Diagnosis
The diagnosis of PH involves a series of tests to rule out other potential causes. Initial assessments include a physical examination, detailed family history, and exposure to drugs. Echocardiography is performed to suggest the presence of PH and detect congenital heart disease. Further tests include ECG, pulmonary function tests, arterial blood gas measurements, and high-resolution CT scans.
Right Heart Catheterisation
Right heart catheterisation remains the gold standard for diagnosing PAH. This invasive procedure measures pulmonary arterial pressure, pulmonary arterial occlusion pressure, and pulmonary vascular resistance.

Treatment
Treatment depends on the type of PH. For PAH, treatments may include high-dose calcium channel blockers for vasoreactive patients, prostacyclin derivatives, endothelin receptor antagonists, PDE-5 inhibitors, and soluble guanylate cyclase activators. Exercise-based rehabilitation improves exercise capacity and quality of life.
Surgical
Surgical options include atrial septostomy, lung transplantation, and pulmonary thromboendarterectomy for chronic thromboembolic pulmonary hypertension.
Monitoring
Patients are monitored through pulse oximetry, arterial blood gas tests, chest X-rays, serial ECG, echocardiography, spirometry, and six-minute walk tests.
Prognosis
The prognosis of PH varies, with untreated PAH having a median survival of 2-3 years. New therapies have improved survival rates, with recent studies showing increased survival times for treated patients.

Epidemiology
Pulmonary hypertension is relatively rare, with an incidence of 4 cases per million worldwide. Women are more frequently affected than men. Other forms of PH are more common, notably in conditions like systemic scleroderma, systemic lupus erythematosus, and sickle cell disease.
Research
Gene therapy is under investigation for inherited forms of the disease.
Self-assessment MCQs (single best answer)
Pulmonary hypertension (PH) is defined by the 6th World Symposium on Pulmonary Hypertension as:

Which of the following is NOT a primary symptom of pulmonary hypertension?
Which group classification of pulmonary hypertension is associated with left heart disease?
What is considered the gold standard for diagnosing pulmonary arterial hypertension (PAH)?
Which of the following is a surgical option for treating chronic thromboembolic pulmonary hypertension?
Pulmonary hypertension is characterised by:
Which of the following conditions is NOT a known risk factor for developing pulmonary hypertension?
Which group of pulmonary hypertension includes idiopathic, heritable, and drug/toxin-induced forms?
What is the median survival time for untreated pulmonary arterial hypertension (PAH)?
Which of the following is NOT a typical physical sign of pulmonary hypertension?
Dentaljuce
Dentaljuce provides Enhanced Continuing Professional Development (CPD) with GDC-approved Certificates for dental professionals worldwide.
Founded in 2009 by the award-winning Masters team from the School of Dentistry at the University of Birmingham, Dentaljuce has established itself as the leading platform for online CPD.
With over 100 high-quality online courses available for a single annual membership fee, Dentaljuce offers comprehensive e-learning designed for busy dental professionals.
The courses cover a complete range of topics, from clinical skills to patient communication, and are suitable for dentists, nurses, hygienists, therapists, students, and practice managers.
Dentaljuce features Dr. Aiden, a dentally trained AI-powered personal tutor available 24/7 to assist with queries and provide guidance through complex topics, enhancing the learning experience.
Check out our range of courses, or sign up now!