Q Fever
Q fever, also known as query fever or coxiellosis, is a disease caused by infection with the bacterium Coxiella burnetii. This organism, although uncommon, can be found in cattle, sheep, goats, and other domestic mammals, including cats and dogs. Human infection typically results from inhalation of spore-like small-cell variants or contact with the milk, urine, faeces, vaginal mucus, or semen of infected animals. The disease is rarely tick-borne. Humans are highly susceptible, and even a few organisms can cause infection. The incubation period ranges from 9 to 40 days.
Signs and Symptoms
The incubation period for Q fever is usually two to three weeks. The most common symptoms are flu-like, including abrupt onset of fever, malaise, profuse sweating, severe headache, muscle pain, joint pain, loss of appetite, and upper respiratory problems. Gastrointestinal symptoms such as nausea, vomiting, and diarrhoea can also occur. Approximately half of infected individuals exhibit no symptoms.
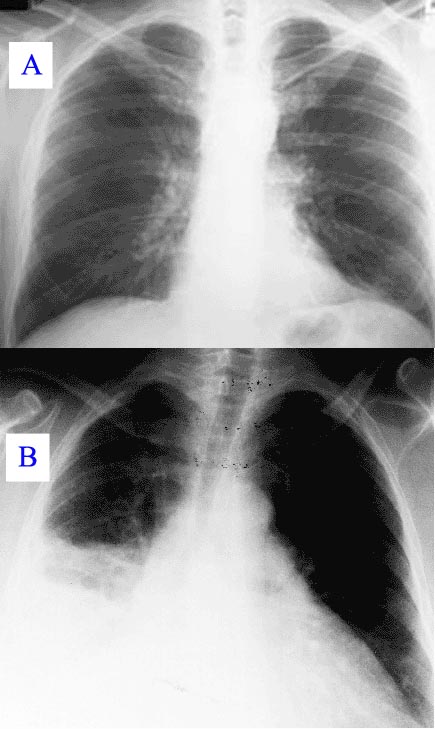
The disease can progress to atypical pneumonia, potentially leading to life-threatening acute respiratory distress syndrome. Less commonly, Q fever can cause granulomatous hepatitis, which may be asymptomatic or present with fever, liver enlargement, and upper right abdominal pain. Chronic Q fever is almost identical to endocarditis and can occur months or decades after initial infection, often proving fatal if untreated. A minority of Q fever survivors develop Q fever fatigue syndrome, characterised by post-exertional malaise and debilitating fatigue, often meeting the diagnostic criteria for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS).
Diagnosis
Diagnosis is typically based on serology, which detects an antibody response rather than the organism itself. Molecular detection of bacterial DNA is increasingly used. Coxiella burnetii can be grown in axenic culture, but this is technically difficult and not routinely available. Q fever can cause endocarditis, which may require transoesophageal echocardiography to diagnose. The definitive diagnosis of Q fever hepatitis is only possible through liver biopsy, showing characteristic fibrin ring granulomas.
Prevention
The first successful Q fever vaccine was developed through research in the 1960s-1970s. Q-Vax, a whole-cell inactivated vaccine developed in Australia, offers protection. Skin and blood tests should be done before vaccination to identify pre-existing immunity. In Australia, a national Q fever vaccination programme was introduced in 2001 for people in high-risk occupations. Vaccination of animals may also be a method of control.
Treatment
Acute Q fever is effectively treated with antibiotics, including doxycycline, tetracycline, chloramphenicol, ciprofloxacin, and ofloxacin. Chronic Q fever is more challenging, requiring prolonged treatment, potentially up to four years, with doxycycline and quinolones or hydroxychloroquine. In pregnancy, where certain antibiotics are contraindicated, co-trimoxazole is preferred.
Epidemiology
Q fever is globally distributed, except for New Zealand and Antarctica. The bacterium is highly virulent and sustainable, with transmission primarily through inhalation of contaminated dust or contact with infected animals. Certain occupations, including veterinary personnel, stockyard workers, farmers, and laboratory workers, pose higher risks for Q fever.

Outbreaks have been reported in Europe, the United States, and other regions, often linked to livestock farming. Proper public health education and interdisciplinary collaboration are essential for developing effective control and prevention strategies.
History
Q fever was first described in 1935 by Edward Holbrook Derrick in Brisbane, Australia. The causative agent, initially identified as a species of Rickettsia, was isolated in 1937 by Frank Macfarlane Burnet and Mavis Freeman. It is now classified as a Gammaproteobacterium, similar to Legionella and Francisella.
Society and Culture
Q fever has appeared in popular culture, including early Dr. Kildare films and the U.S. television medical drama House.
Biological Warfare
C. burnetii has been investigated as a potential biological warfare agent due to its high infectivity and stability in aerosols. The CDC ranks it as a "category B" bioterrorism agent.
In Animals
Q fever affects various domestic and wild animals, primarily causing reproductive issues in ruminants like cattle, sheep, and goats. The disease is present worldwide, except New Zealand. Biosecurity measures and vaccination are very important for controlling Q fever in animal populations and reducing human infection risks.
Self-assessment MCQs (single best answer)
What is the primary cause of Q fever?

How is Q fever most commonly transmitted to humans?
What is the typical range for the incubation period of Q fever?
Which of the following symptoms is least associated with acute Q fever?
What is the definitive method for diagnosing Q fever hepatitis?
Which antibiotic is commonly used in the treatment of acute Q fever?
Which country has a national Q fever vaccination programme for high-risk occupations?
What is the primary method of Q fever prevention in animals?
Who first described Q fever in 1935?
Which category of bioterrorism agent does the CDC classify Coxiella burnetii as?
Dentaljuce
Dentaljuce provides Enhanced Continuing Professional Development (CPD) with GDC-approved Certificates for dental professionals worldwide.
Founded in 2009 by the award-winning Masters team from the School of Dentistry at the University of Birmingham, Dentaljuce has established itself as the leading platform for online CPD.
With over 100 high-quality online courses available for a single annual membership fee, Dentaljuce offers comprehensive e-learning designed for busy dental professionals.
The courses cover a complete range of topics, from clinical skills to patient communication, and are suitable for dentists, nurses, hygienists, therapists, students, and practice managers.
Dentaljuce features Dr. Aiden, a dentally trained AI-powered personal tutor available 24/7 to assist with queries and provide guidance through complex topics, enhancing the learning experience.
Check out our range of courses, or sign up now!